Results of Intraoperative Manual Cyclotorsion Compensation for Myopic Astigmatism in Patients Undergoing Small Incision Lenticule Extraction (SMILE)
|
|
|
- Abigail Armstrong
- 6 years ago
- Views:
Transcription
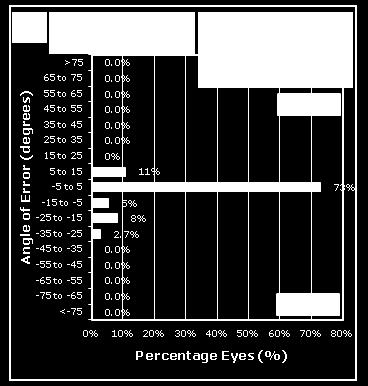
1 ORIGINAL ARTICLE Results of Intraoperative Manual Cyclotorsion Compensation for Myopic Astigmatism in Patients Undergoing Small Incision Lenticule Extraction (SMILE) Sri Ganesh, MS, DNB; Sheetal Brar, MS, DNB; Archana Pawar, MS ABSTRACT PURPOSE: To study the safety, efficacy, and outcomes of manual cyclotorsion compensation in small incision lenticule extraction (SMILE) for myopic astigmatism. METHODS: Eligible patients with myopia from to diopters (D) spherical equivalent with a minimum astigmatism of 0.75 D undergoing SMILE were included. Intraoperative cyclotorsion compensation was performed by gently rotating the cone and aligning the 0 to 180 limbal marks with the horizontal axis of the reticule of the right eye piece of the microscope of the femtosecond laser after activating the suction. RESULTS: In this study, 81 left eyes from 81 patients were analyzed for vector analysis of astigmatism. The mean cyclotorsion was 5.64 ± 2.55 (range: 2 to 12 ). No significant differences were found for surgically induced astigmatism, difference vector, angle of error (AE), correction index, magnitude of error, index of success (IOS), and flattening index between 2 weeks and 3 months postoperatively (P >.05). The eyes were categorized into low ( 1.50 D, n = 37) and high (> 1.50 D, n = 44) cylinder groups. At 3 months, intergroup analysis showed a comparable correction index of 0.97 for the low and 0.93 for the high cylinder groups, suggesting a slight undercorrection of 3% and 7%, respectively (P =.14). However, the AE and IOS were significantly lower in the high compared to the low cylinder group (P =.032 and.024 for AE and IOS, respectively), suggesting better alignment of the treatment in the high cylinder group. However, the mean uncorrected distance visual acuity of both groups was comparable (P =.21), suggesting good visual outcomes in the low cylinder group despite a less favorable IOS. CONCLUSIONS: Manual compensation may be a safe, feasible, and effective approach to refine the results of astigmatism with SMILE, especially in higher degrees of cylinders. [J Refract Surg. 2017;33(8): ] T he refractive outcome of astigmatism correction has been shown to depend on the accuracy of the axis treatment. Any rotational movement of the eye (cyclotorsion) during treatment may cause a shift in the treatment axis, leading to undesirable results such as undercorrection and induction of aberrations. 1-3 Most of the currently available excimer laser platforms have the ability to detect and compensate for the static and dynamic cyclotorsion due to positional changes and treatment by advanced software and eye tracking. 1,4 Active cyclotorsion error correction in LASIK improved the accuracy of cylinder correction. 4-6 Although there are numerous studies on cyclotorsion and its compensation in LASIK, significant data do not exist for the small incision lenticule extraction (SMILE) procedure. Studies on femtosecond lenticule extraction and SMILE have shown significant undercorrection of astigmatism over time. 7-9 The probable explanation of these results could be the unavailability of an active eye tracking software in the VisuMax femtosecond laser system (Carl Zeiss Meditec, Jena, Germany) used to perform these procedures. Because no definite method of cyclotorsion compensation exists for SMILE, this may also be considered a potential limitation of this procedure. Previous studies on LASIK suggested that manual markings were equally safe and effective as the automated dynamic eye trackers for cyclotorsion compensation during surgery. 10 Based on these observations, we attempted to investigate the feasibility of manual compensation for the intraoperative torsional error by using limbal markings as a guide in patients undergoing SMILE for myopic astigmatism. We describe a simple and practical method for the manual compensation of cyclotorsion during SMILE in patients with From Nethradhama Superspeciality Eye Hospital, Bengaluru, Karnataka, India. Submitted: July 27, 2016; Accepted: February, 3, 2017 The authors have no financial or proprietary interest in the materials presented herein. Correspondence: Sheetal Brar, MS, DNB, Nethradhama Superspeciality Eye Hospital, 256/14, Kanakapura Main Road, 7th Block, Jayanagar, Bengaluru, Karnataka , India. brar_sheetal@yahoo.co.in doi: / x Copyright SLACK Incorporated
2 Manual Cyclotorsion Compensation/Ganesh et al significant myopic astigmatism (> 0.75 diopters [D]). We evaluated the safety, efficacy, and reliability of this technique in terms of cylindrical correction and postoperative refractive outcomes in a prospective, interventional study with 3-month follow-up. PATIENTS AND METHODS This prospective, nonrandomized study was approved by our institutional ethics committee and adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients participating in the study. Inclusion criteria were age between 21 and 40 years, myopic astigmatism with up to D spherical equivalent (SE) with a minimum astigmatism of 0.75 D, stable refraction (< 0.50 D change in the past 12 months), corrected distance visual acuity (CDVA) of 20/30 or better, healthy ocular surface, absence of corneal ectatic diseases, corneal scars, absence of any retinal pathology likely to affect visual outcomes, and ensured follow-up visits. Eyes with thin corneas (central corneal thickness < 480 µm), diagnosed or suspicious cases of corneal ectatic conditions, severe dry eyes, and contact lens induced allergy, patients taking systemic steroids, immunosuppressants, oral contraceptives, or antidepressants, and pregnant females were excluded from the study. Preoperative Evaluation All patients underwent a thorough preoperative evaluation including anterior and posterior segment examination, cycloplegic and subjective refraction, assessment of uncorrected distance visual acuity (UDVA) and CDVA, corneal topography using the Pentacam HR (Oculus Optikgeräte GmbH, Wetzlar, Germany) and Orbscan II (Bausch & Lomb, Rochester, NY), contrast sensitivity using the Functional Acuity Contrast Test (F.A.C.T. Stereo Optical Co., Inc., Chicago, IL), aberrometry (Hoya itrace Surgical Workstation; Hoya Surgical Optics, Tokyo, Japan), specular microscopy (Tomey, Nagoya, Japan), and dry eye evaluation (Schirmer 1 and tear film break-up time). Patients using soft or rigid contact lenses were instructed to discontinue their lenses at least 1 and 3 weeks, respectively, prior to the topographic evaluation. Treatment Planning Regardless of the degree of myopia, a 10% overcorrection nomogram was applied to both the spherical and cylindrical components of the refractive error for all eyes. Journal of Refractive Surgery Vol. 33, No. 8, 2017 Surgical Technique All surgeries were performed by a single experienced refractive surgeon (SG) under topical anesthesia using the VisuMax femtosecond laser, with a pulse repetition rate of 500 khz, cut energy of 160 nj with a spot separation of 4.5 µm, 6.5- to 7-mm optical zone, cap thickness of 120 µm, and 2-mm superior incision. The treatment was centered on the visual axis. Mean optical zone used was 6.50 ± 0.23 mm. Preoperatively, the limbus was marked in the 0 to 180 axis with a dye permitting the transmission of infrared radiation (Viscot surgical skin marker 1436; Viscot Medical, East Hanover, NJ) using either a marker pen or Ganesh bubble marker (Epsilon Surgical, Chino, CA) (Figure A, available in the online version of this article) in the upright position. The patient was then positioned under the VisuMax femtosecond laser and instructed to look into the green flashing fixation light. Once proper centration was achieved, the eye was docked to the patient interface and suction was applied. The extent of cyclotorsion, if any, was determined using the reticule (present in the right eyepiece) and any cyclotorsion (incyclotorsion or excyclotorsion) was manually compensated for by gently rotating the contact glass to align the horizontal marks on the eye to the 0 to 180 axis of the reticule (Figure A and Video 1, available in the online version of this article). Once both were aligned, the active laser process was started to create the refractive lenticule. After lenticule creation by the femtosecond laser, the anterior and posterior lenticule planes were dissected using a blunt dissector, followed by lenticule extraction through the side cut. The interface was washed with balanced salt solution. Postoperative medications included topical 0.3% ofloxacin (Exocin; Allergan, Irvine, CA) four times for 3 days, 0.1% prednisolone acetate eye drops (Pred Forte; Allergan) in tapering dosage for 4 weeks, and lubricants four times for 4 weeks or more. All surgeries were uneventful and no complications such as suction loss, black spots, difficult dissection, or incomplete separation of lenticule due to the ink marks blocking the laser occurred in any of the eyes. Patients were followed up at postoperative 1 day, 2 weeks, and 3 months. On all follow-up visits from 2 weeks on, assessment of UDVA, manifest refraction, CDVA, and topography were also performed. Statistical Analysis SPSS for Windows software (version ; IBM Corporation, Armonk, NY) was used for statistical analysis. All values were expressed as mean ± standard deviation (SD). The independent samples t test was performed for intergroup comparison and the paired t test was used for intragroup comparison of means. A P value of.05 or less was considered statistically significant. Standard refractive graphs were 507
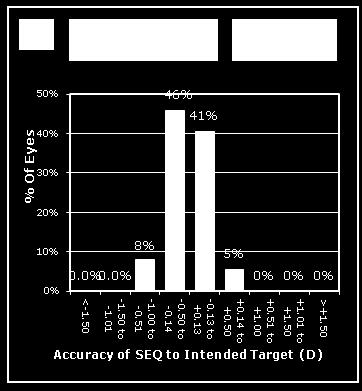
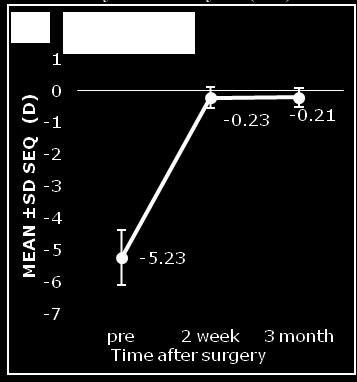
3 Manual Cyclotorsion Compensation/Ganesh et al TABLE 1 Preoperative Baseline Characteristics of Patients (N = 81) a Characteristic Total (N = 81) Low Cylinder (n = 37) High Cylinder (n = 44) P Age (y) ± ± ± SE (D) ± ± ± Cylinder (D) ± ± ± UDVA (logmar) 0.76 ± ± ± CDVA (logmar) ± ± ± Intraoperative cyclotorsion 5º 81.6% 75.67% 86.36% 6 to 9º 17.2% 21.62% 13.63% 10º 1.2% 2.7% 0% Mean ± SD 5.64 ± ± ± Range 2 to 12 2 to 12 2 to 10 SE = spherical equivalent; D = diopters; UDVA = uncorrected distance visual acuity; CDVA = corrected distance visual acuity; SD = standard deviation a Values given as mean ± SD unless otherwise noted. b Calculated between the low and high cylinder groups. generated using Datagraph-med 5.20 software ( Vector Analysis of Astigmatism Only the left eyes were included in the analysis. Astigmatism outcomes were reported according to the standardized format Refractive astigmatism at the spectacle plane was converted to the corneal plane using a vertex distance of 12 mm. It was then analyzed with the vector analysis of Alpins using the Assort software (ASSORT Pty. Ltd., Victoria, Australia), with consideration of the change in the astigmatic axis, measuring three vectors and relationships among them. Target induced astigmatism vector (TIA) was defined as the astigmatic change that the surgery was intended to induce, surgically induced astigmatism vector (SIA) was defined as the astigmatic change that the surgery actually induced, and the difference vector (DV) was defined as the induced astigmatic change that would enable the initial surgery to achieve its intended target or the postoperative astigmatism. Magnitude of error (ME) is the arithmetic difference between the SIA and TIA. Angle of error (AE) is the angle between the axis of the SIA and TIA. The flattening index (FI) is a measure of the impact of an astigmatic treatment at off-axis orientation on the astigmatic change at its intended axis. RESULTS A total of 81 left eyes from 81 patients were analyzed. The eyes were categorized into low ( 1.50 D, n = 37) and high (> 1.50 D, n = 44) cylinder groups, based on the magnitude of preoperative astigmatism. The preoperative patient characteristics are given in Table 1. Incyclotorsion was more commonly observed (44% of eyes) compared to excyclotorsion (38% of eyes), whereas 18% of eyes did not show any cyclotorsion. However, for convenience of analysis, both incyclotorsion and excyclotorsion were considered broadly as cyclotorsion and separate results were not analyzed for incyclotorsion and excyclotorsion. Overall, the average cyclotorsion observed was 5.64 ± 2.55 (range: 2 to 12 ). The magnitude of cyclotorsion was 5 or less in 81%, between 6 and 10 in 17.6%, and 10 or greater in 1.2% of eyes. The mean cyclotorsion was comparable in both the low (5.73 ± 2.8 ) and high (5.53 ± 2.29 ) cylinder groups, with no statistically significant difference between their values (P =.822) (Table 1). Visual Outcomes The mean UDVA showed significant improvement in both groups from 2 weeks to 3 months postoperatively (P <.05 for both groups). However, there was no statistically significant improvement in CDVA in either group over time (Table A, available in the online version of this article). Efficacy (Postoperative UDVA/Preoperative CDVA) All eyes had UDVA of 20/32 or better at 3 months, with 84% eyes with UDVA of 20/20 or better (Figure 1). However, the percentage of eyes achieving UDVA of 20/20 or better was higher in the low (95%) versus the high (75%) cylinder group (Figures B-C, available in the online version of this article). 508 Copyright SLACK Incorporated


 Overall, 56% eyes gained one")
.")
 compared to the low cylinder group")




.")


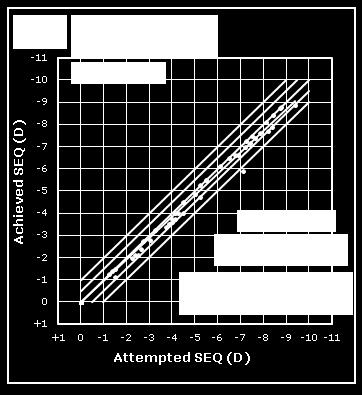
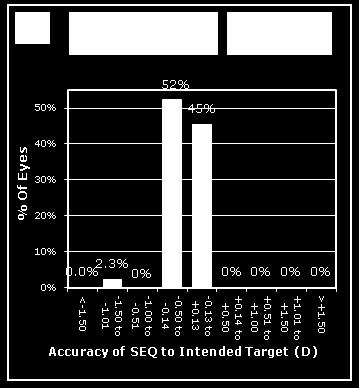
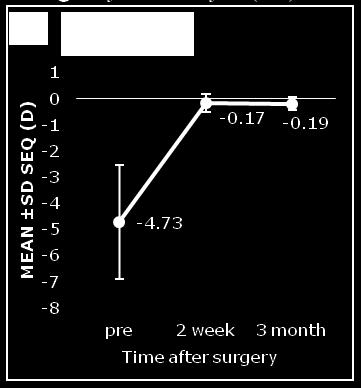
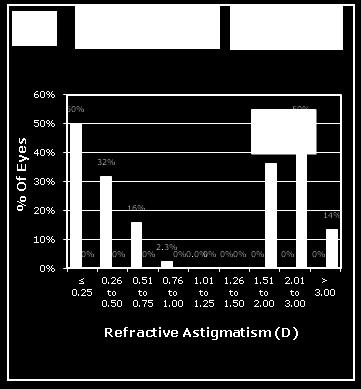
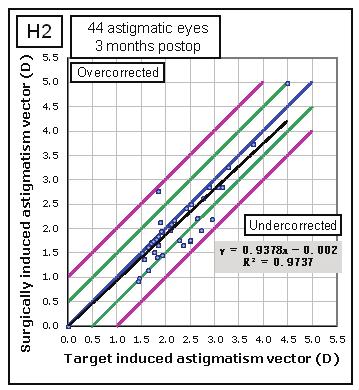
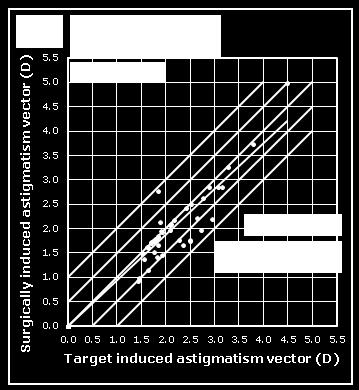
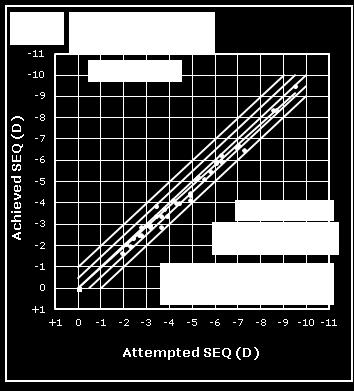
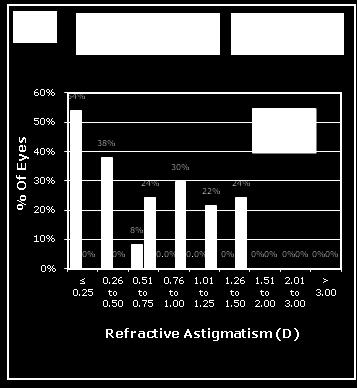
4 Manual Cyclotorsion Compensation/Ganesh et al Figure 1. Standard graphs for visual outcomes for total eyes. UDVA = uncorrected distance visual acuity; CDVA = corrected distance visual acuity; D = diopters; SEQ = spherical equivalent refraction Safety (Postoperative CDVA/Preoperative CDVA) Overall, 56% eyes gained one or more lines of CDVA at the end of the 3-month follow-up (Figure 1). In the high cylinder group, the gain in CDVA was greater (60%) compared to the low cylinder group (54%) (Figures B-C). No eye in either group had loss of CDVA compared to preoperative corrected vision. Refractive Outcomes The mean SE reduced from ± 2.18 D preoperatively to ± 0.24 D at the end of the 3-month Journal of Refractive Surgery Vol. 33, No. 8, 2017 follow-up (P =.000). A total of 95% eyes were within ±0.50 D, whereas all eyes were within ±1.50 D of SE correction (Figure 2, Table A). Overall, the predictability of cylinder correction was excellent, with all eyes within ±1.00 D of astigmatism correction at 3 months (Figure 2). However, the predictability was slightly better in the low (average deviation: D) versus the high (average deviation: D) cylinder group, indicating more undercorrection of astigmatism treatment in the latter group (Figure 2). 509
 total (N = 81 eyes), (B) low cylinder (n = 37 eyes), and (C) high cylinder (n = 44 eyes) groups. Above the white line in the middle is overcorrection and below is undercorrection.")
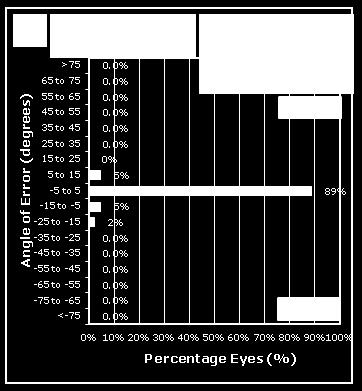
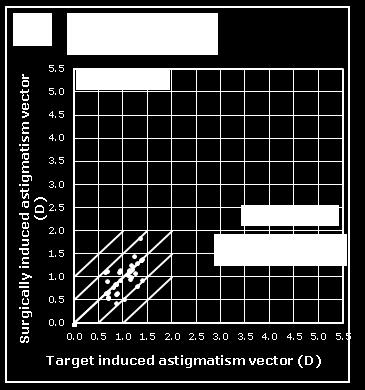
5 Manual Cyclotorsion Compensation/Ganesh et al Figure 2. Predictability scatter (attempted vs achieved) of cylindrical refraction with small incision lenticule extraction (SMILE) at 3 months. Data for (A) total (N = 81 eyes), (B) low cylinder (n = 37 eyes), and (C) high cylinder (n = 44 eyes) groups. Above the white line in the middle is overcorrection and below is undercorrection. The red solid line indicates the outcome of linear regression analysis. A B Figure 3. Index of success (IOS) for (A) low cylinder and (B) high cylinder groups at 3 months. The postoperative SE and cylinder remained fairly stable, with no significant difference between 2 weeks and 3 months (P >.05) (Figure 1, Figures B-C). Vector Analysis The vector analysis results of the 81 eyes using 2-week and 3-month refractive data are shown in Tables B-C (available in the online version of this article). No significant differences were found for SIA, DV, AE, correction index (CI), ME, IOS, and FI between 2 weeks and 3 months (P >.05). Intergroup analysis at 3 months showed that there was no significant difference between the low and high cylinder groups in terms of the DV, CI, ME, and FI. However, the absolute AE and IOS was significantly higher in the low cylinder compared to the high cylinder group (P =.032 and.024 for AE and IOS, respectively) (Figure 3). On the other hand, the ME was higher in the high cylinder compared to the low cylinder group (P =.032) (Tables B-C). DISCUSSION Previous studies evaluating astigmatism correction showed superior results with femtosecond laser assisted LASIK compared to SMILE. 14,15 Chan et al. 14 showed that the alignment of treatment was more variable in SMILE, leading to a lower efficacy compared to LASIK at 3 months in eyes with low to moderate myopic astigmatism. Ivarsen et al. 16 demonstrated a significant undercorrection of astigmatism and an increased error of treatment with higher attempted cylinder correction. The reported undercorrection was 13% per diopter of attempted cylinder correction in low astigmatic and 16% per diopter in highly astigmatic eyes. This was mainly attributed to noncompensation of errors of cyclotorsion and nonapplication of nomograms during the procedure. However, in contrast to the study by Ivarsen et al., improved results for astigmatism treatment were achieved in the current study with SMILE. Because we 510 Copyright SLACK Incorporated
6 Manual Cyclotorsion Compensation/Ganesh et al attempted the compensation of cyclotorsion manually and also applied a 10% nomogram (based on the postoperative results of our initial cases of SMILE, which showed undercorrection of up to 1.00 D), the accuracy of astigmatism correction observed was far better compared to the results reported in previous studies This was indicated by the high CIs of 0.97 and 0.93 for the low and high cylinder groups, respectively, suggesting an undercorrection of 3% and 7%, respectively, which is approximately 0.25 D, at 3 months. One reason for more undercorrection in the high cylinder group may be a lower mean age compared to the low cylinder group; hence patients in this group were younger with different corneal biomechanics and epithelial healing patterns, which could have given rise to the undercorrection. 17 Also, higher degrees of cylinders were shown to have a tendency for greater undercorrection over time. 16 However, from a clinical point of view, slight undercorrection would be preferred to overcorrection because a change in the direction of the cylinder axis would probably be poorly accepted by patients. Although the CI was close to 1 (0.97), the IOS had a higher and thus less favorable numerical value than the high cylinder group, indicating greater misalignment in the low cylinder group. Although the absolute AE and IOS were significantly higher in the low cylinder group compared to the high cylinder group, indicating a suboptimal correction of astigmatism, the visual outcomes in terms of UDVA were similar in both groups at 3 months. This may suggest that it may not be compulsory to manually correct for cyclotorsion in lower degrees of astigmatism in SMILE. The accuracy of treatment of lower degrees of astigmatism would depend on various factors, such as the reliability of preoperative measurement of the magnitude and axis of the cylinder and manual marking, and also assessment of the extent of intraoperative cyclotorsion. Therefore, the advantages of manual compensation in low cylinders may not be ascertained, especially if the intraoperative cyclotorsion is less (< 5 ). However, it may have a definite advantage in moderate to high degrees of astigmatism because even minimal meridional errors may have significant negative refractive consequences. 18 In this study, the magnitude of intraoperative cyclotorsion was 5 or less in most eyes (81.6%). However, rotation of greater than 5 was found in 18.4% of eyes and 10 or greater in 1.2% of eyes. Studies have shown that rotation of 5 or greater can induce significant undercorrection of the astigmatic component of the refraction and that undercorrection is more noticeable as the degree of astigmatism increases. 19,20 Hence, based on the results of this study, we recommend manual compensation of cyclotorsion error for all eyes with high astigmatism (> 1.50 D) with any degree of cyclotorsion and low astigmatism ( 1.50 D) with 5 or greater, using the technique described. In terms of flattening effect achieved, our study showed better FI (0.93) at 3 months compared to the study by Kobashi et al., 21 which showed insufficient flattening with both femtosecond lenticule extraction and SMILE (median flattening indices of 0.79 to 0.80). There were two potential limitations to this study. First, we did not compare our results with a control group without cyclotorsion compensation. This was done on ethical grounds because we had observed some cases with suboptimal outcomes with high cylinders, and after using this technique our outcomes with astigmatism improved significantly. Second, we determined the postoperative astigmatism at 3 months, when the corneal shape was considered to have been stabilized, taking into account the wound healing responses of the cornea. However, a longer follow-up may be desirable to evaluate the long-term stability of the results obtained with this technique. Also, we did not study the corneal aberrations and their relationship with cylinder undercorrection. The main purpose of the study was to report the outcomes with the technique of manual compensation for cyclotorsion in SMILE because, to the authors knowledge, this has not been reported earlier. In addition, we wanted to analyze the results of vector analysis of astigmatism with this technique for low cylinder ( 1.50 D) and high cylinder (> 1.50 D) eyes, and provide future recommendations for using this technique based on our experience. Nevertheless, to the best of our knowledge, this is the first preliminary report on the outcomes of astigmatism correction in SMILE using manual compensation. In our experience, gentle rotation of the cone does not lead to loss of suction and no complications occur due to limbal marking. Hence, it may be a safe, simple, and effective approach to improve results of astigmatism with SMILE in the absence of an active eye tracker in the current version of the VisuMax femtosecond laser. However, prospective randomized controlled studies with a longer follow-up may be necessary to confirm the validity of our results. AUTHOR CONTRIBUTIONS Study concept and design (SG); data collection (AP); analysis and interpretation of data (SB, AP); writing the manuscript (SB, AP); critical revision of the manuscript (SG, SB); administrative, technical, or material support (SG) Journal of Refractive Surgery Vol. 33, No. 8,
7 Manual Cyclotorsion Compensation/Ganesh et al REFERENCES 1. Febbraro JL, Koch D, Khan HN, Saad A, Gatinel D. Detection of static cyclotorsion and compensation for dynamic cyclotorsion in laser in situ keratomileusis. J Cataract Refract Surg. 2010;36: Swami AU, Steinert RF, Osborne WE, White AA. Rotational malposition during laser in situ keratomileusis. Am J Ophthalmol. 2002;133: Arba-Mosquera S, Merayo-Lloves J, de Ortueta D. Clinical effects of pure cyclotorsional errors during refractive surgery. Invest Ophthalmol Vis Sci. 2008;49: Reinstein DZ, Gobbe M, Gobbe L, Archer TJ, Carp GI. Optical zone centration accuracy using corneal fixation-based SMILE compared to eye tracker-based femtosecond laser-assisted LASIK for myopia. J Refract Surg. 2015;31: Aslanides IM, Toliou G, Padroni S, Arba Mosquera S, Kolli S. The effect of static cyclotorsion compensation on refractive and visual outcomes using the Schwind Amaris laser platform for the correction of high astigmatism. Cont Lens Anterior Eye. 2011;34: Lazaridis A, Droutsas K, Sekundo W. Topographic analysis of the centration of the treatment zone after SMILE for myopia and comparison to FS-LASIK: subjective versus objective alignment. J Refract Surg. 2014;30: Kunert KS, Russmann C, Blum M, Sluyterman WG. Vector analysis of myopic astigmatism corrected by femtosecond refractive lenticule extraction. J Cataract Refract Surg. 2013;39: Blum M, Kunert KS, Engelbrecht C, Dawczynski J, Sekundo W. Femtosecond lenticule extraction (FLEx): results after 12 months in myopic astigmatism [article in German]. Klin Monbl Augenheilkd. 2010;227: Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6-month prospective study. Br J Ophthalmol. 2011;95: Shen EP, Chen WL, Hu FR. Manual limbal markings versus irisregistration software for correction of myopic astigmatism by laser in situ keratomileusis. J Cataract Refract Surg. 2010;36: Alpins NA. A new method of analyzing vectors for changes in astigmatism. J Cataract Refract Surg. 1993;19: Alpins NA. New method of targeting vectors to treat astigmatism. J Cataract Refract Surg. 1997;23: Alpins NA. Vector analysis of astigmatism changes by flattening, steepening, and torque. J Cataract Refract Surg. 1997;23: Chan TC, Ng AL, Cheng GP, et al. Vector analysis of astigmatic correction after small-incision lenticule extraction and femtosecond-assisted LASIK for low to moderate myopic astigmatism. Br J Ophthalmol. 2016;100: Zhang J, Wang Y, Wu W, Xu L, Li X, Dou R. Vector analysis of low to moderate astigmatism with small incision lenticule extraction (SMILE): results of a 1-year follow-up. BMC Ophthalmol. 2015;15: Ivarsen A, Asp S, Hjortdal J. Safety and complications of more than 1500 small-incision lenticule extraction procedures. Ophthalmology. 2014;121: Sharifipour F, Panahi-Bazaz M, Bidar R, Idani A, Cheraghian B. Age-related variations in corneal biomechanical properties. J Curr Ophthalmol. 2016;28: Febbraro J-L, Aron-Rosa D, Gross M, Aron B, Brémond-Gignac D. One year clinical results of photoastigmatic refractive keratectomy for compound myopic astigmatism. J Cataract Refract Surg. 1999;25: Tjon-Fo-Sang MJ, de Faber JT, Kingma C, Beekhuis WH. Cyclotorsion: a possible cause of residual astigmatism in refractive surgery eye motion occurring between wavefront measurement and refractive surgery. J Cataract Refract Surg. 2002;28: Chernyak DA. Cyclotorsion eye motion occurring between wavefront measurement and refractive surgery. J Cataract Refract Surg. 2004;30: Kobashi H, Kamiya K, Ali MA, Igarashi A, Elewa MEM, Shimizu K. Comparison of astigmatic correction after femtosecond lenticule extraction and small incision lenticule extraction for myopic astigmatism. PloS One. 2015;10:e Miao H, Tian M, Xu Y, Chen Y, Zhou X. Visual outcomes and optical quality after femtosecond laser small incision lenticule extraction: an 18-month prospective study. J Refract Surg. 2015;31: Ganesh S, Gupta R. Comparison of visual and refractive outcomes following femtosecond laser-assisted LASIK with SMILE in patients with myopia or myopic astigmatism. J Refract Surg. 2014;30: Copyright SLACK Incorporated

8 Figure A. (A) Preoperative limbal marking with the Ganesh bubble marker (Epsilon Surgical, Chino, CA) under topical anesthesia in the upright position. This instrument uses three marks on the limbus at 0, 90, and 180, extending 2 mm toward the center of the cornea, which are easy to visualize while the eye is being docked. (B) Method of manual cyclotorsion compensation by a gentle rotation of the cone while holding the same at the attachment of the tube to the cone. (C) Position of the limbal marks (red arrows) under suction ON condition without cyclotorsion compensation before starting the laser, showing approximately 12 of cyclotorsion. (D) Final position of the limbal marks after manual compensation of the cyclotorsion error (alignment with the horizontal axis of the eyepiece reticule). Delivery of the laser follows this.
9 TABLE A Visual and Refractive Results a Group Preoperative 2 Weeks Postoperative 3 Months Postoperative Total (N = 81) UDVA (logmar) 0.76 ± ± ± 0.08 P b CDVA (logmar) ± ± ± 0.07 P b SE (D) ± ± ± 0.24 Range to to to 0.50 P b Cylinder (D) ± ± ± 0.30 Range to to to 0.50 P b Low cylinder (n = 37) UDVA (logmar) 0.73 ± ± ± 0.07 P b CDVA (logmar) ± ± ± 0.08 P b SE (D) ± ± ± 0.25 Range to to to 0.50 P b Cylinder (D) ± ± ± 0.30 Range to to to 0.50 P b High cylinder (n = 44) UDVA (logmar) 0.78 ± ± ± 0.08 P b CDVA (logmar) ± ± ± 0.06 P b SE (D) ± ± ± 0.24 Range to to to 0.00 P b Cylinder (D) ± ± ± 0.31 Range to to to 0.00 P b High/low cylinder UDVA (P) c CDVA (P) c UDVA = uncorrected distance visual acuity; CDVA = corrected distance visual acuity; SE = spherical equivalent; D = diopters a Values given as mean ± standard deviation unless otherwise noted. b Paired samples t test. c Independent samples t test.





10 Figure B. Standard graphs for visual outcomes for high cylinder eyes. UCVA = uncorrected distance visual acuity; CDVA = corrected distance visual acuity; D = diopters; SEQ = spherical equivalent refraction





11 Figure C. Standard graphs for visual outcomes for low cylinder eyes. UDVA = uncorrected distance visual acuity; CDVA = corrected distance visual acuity; D = diopters; SEQ = spherical equivalent refraction
12 TABLE B Vector Analysis of Total (N = 81) Eyes Undergoing SMILE With Manual Cyclotorsion Compensation Postoperatively Parameter 2 Weeks Postoperative 3 Months Postoperative P SIA 1.53 ± ± DV 0.33 ± ± CI 0.95 ± ± AE (absolute) 4.09 ± ± ME ± ± IOS 0.24 ± ± FI 0.92 ± ± SMILE = small incision lenticule extraction; SIA = surgically induced astigmatism; DV = difference vector; CI = correction index; AE = angle of error; ME = magnitude of error; IOS = index of success; FI = flattening index TABLE C Subgroup Analysis of Astigmatic Correction Based on Degree of Target-Induced Astigmatism After SMILE Parameter Low Cylinder (n = 37) High Cylinder (n = 44) P TIA (preoperative) 0.99 ± ± SIA 0.98 ± ± DV 0.25 ± ± CI 0.97 ± ± AE (absolute) 5.27 ± ± ME ± ± IOS 0.27 ± ± FI 0.96 ± ± SMILE = small incision lenticule extraction; TIA = target induced astigmatism; SIA = surgically induced astigmatism; DV = difference vector; CI = correction index; AE = angle of error; ME = magnitude of error; IOS = index of success; FI = flattening index
ORIGINAL ARTICLE. Primary Topography-Guided LASIK: Treating Manifest Refractive Astigmatism Versus Topography-Measured Anterior Corneal Astigmatism
 ORIGINAL ARTICLE Primary Topography-Guided LASIK: Treating Manifest Refractive Astigmatism Versus Topography-Measured Anterior Corneal Astigmatism Avi Wallerstein, MD, FRCSC; Mathieu Gauvin, BEng, PhD;
ORIGINAL ARTICLE Primary Topography-Guided LASIK: Treating Manifest Refractive Astigmatism Versus Topography-Measured Anterior Corneal Astigmatism Avi Wallerstein, MD, FRCSC; Mathieu Gauvin, BEng, PhD;
Clinical outcomes of Transepithelial photorefractive keratectomy to treat low to moderate myopic astigmatism
 Xi et al. BMC Ophthalmology (2018) 18:115 https://doi.org/10.1186/s12886-018-0775-5 RESEARCH ARTICLE Clinical outcomes of Transepithelial photorefractive keratectomy to treat low to moderate myopic astigmatism
Xi et al. BMC Ophthalmology (2018) 18:115 https://doi.org/10.1186/s12886-018-0775-5 RESEARCH ARTICLE Clinical outcomes of Transepithelial photorefractive keratectomy to treat low to moderate myopic astigmatism
Standard for Reporting Refractive Outcomes of Intraocular Lens Based Refractive Surgery
 EDITORIAL Standard for Reporting Refractive Outcomes of Intraocular Lens Based Refractive Surgery Dan Z. Reinstein, MD, MA(Cantab), FRCSC; Timothy J. Archer, MA(Oxon), DipCompSci(Cantab); Sathish Srinivasan,
EDITORIAL Standard for Reporting Refractive Outcomes of Intraocular Lens Based Refractive Surgery Dan Z. Reinstein, MD, MA(Cantab), FRCSC; Timothy J. Archer, MA(Oxon), DipCompSci(Cantab); Sathish Srinivasan,
DOWNLOAD ASTIGMATIC TECHNIQUE IN ONE STEP RAINBOW HOLOGRAPHY
 ASTIGMATIC TECHNIQUE IN ONE PDF DOWNLOAD 1 / 5 2 / 5 3 / 5 astigmatic technique in one pdf astigmatic technique in one pdf Signs and symptoms. Although astigmatism may be asymptomatic, higher degrees of
ASTIGMATIC TECHNIQUE IN ONE PDF DOWNLOAD 1 / 5 2 / 5 3 / 5 astigmatic technique in one pdf astigmatic technique in one pdf Signs and symptoms. Although astigmatism may be asymptomatic, higher degrees of
Novel Microscope Mounted Digital Keratoscope for Intra-Operative Toric IOL Alignment
 Cronicon OPEN ACCESS EC OPHTHALMOLOGY Research Article Novel Microscope Mounted Digital Keratoscope for Intra-Operative Toric IOL Alignment Sviatlana M Ilyina 1 *, Siarhei M Lohash 2 and Alex Artsyukhovich
Cronicon OPEN ACCESS EC OPHTHALMOLOGY Research Article Novel Microscope Mounted Digital Keratoscope for Intra-Operative Toric IOL Alignment Sviatlana M Ilyina 1 *, Siarhei M Lohash 2 and Alex Artsyukhovich
Disclosure. Getting Up to Date with LASIK. Modern advancements LASIK. What we re curing. Changing the corneal surface
 Getting Up to Date with LASIK Disclosure I am not a paid consultant to any drug or device company. Stillwater, MN Adjunct Associate Professor University of Minnesota LASIK Use one instrument to make a
Getting Up to Date with LASIK Disclosure I am not a paid consultant to any drug or device company. Stillwater, MN Adjunct Associate Professor University of Minnesota LASIK Use one instrument to make a
Non-penetrating Femtosecond Laser. intrastromal astigmatic keratotomy (ISAK) Patients With Mixed Astigmatism After Previous Refractive Surgery
 Patients With Mixed Astigmatism After Previous Refractive Surgery") ORIGINAL ARTICLE Non-penetrating Femtosecond Laser Intrastromal Astigmatic Keratotomy in Patients With Mixed Astigmatism After Previous Refractive Surgery Jan Venter, MD; Rodney Blumenfeld, MD; Steve Schallhorn,
ORIGINAL ARTICLE Non-penetrating Femtosecond Laser Intrastromal Astigmatic Keratotomy in Patients With Mixed Astigmatism After Previous Refractive Surgery Jan Venter, MD; Rodney Blumenfeld, MD; Steve Schallhorn,
Abstract. imedpub Journals Vol.3 No.2:27. Introduction
 Research Article imedpub Journals http://www.imedpub.com/ Journal of Eye & Cataract Surgery DOI: 10.21767/2471-8300.100027 Intraoperative Biometry versus Conventional Methods for Predicting Intraocular
Research Article imedpub Journals http://www.imedpub.com/ Journal of Eye & Cataract Surgery DOI: 10.21767/2471-8300.100027 Intraoperative Biometry versus Conventional Methods for Predicting Intraocular
* Villegas EL, Alcón E, Artal P. Minimum amount of astigmatism that should be corrected. J Cataract Refract Surg 2014; 40: n My SIA: Ø Centroid
 Astigmatism correction in cataract surgery: A work in progress 9 things you should know Douglas D. Koch, M.D. Cullen Eye Institute Baylor College of Medicine Houston, Texas Financial disclosure: AMO Alc
Astigmatism correction in cataract surgery: A work in progress 9 things you should know Douglas D. Koch, M.D. Cullen Eye Institute Baylor College of Medicine Houston, Texas Financial disclosure: AMO Alc
LASIK for post penetrating keratoplasty astigmatism and myopia
 Br J Ophthalmol 1999;83:113 118 113 The Eye Institute, Chatswood, NSW, Australia S K Webber M A Lawless G L Sutton C M Rogers Correspondence to: Dr Michael Lawless, Level 3, 7 Victoria Avenue, Chatswood,
Br J Ophthalmol 1999;83:113 118 113 The Eye Institute, Chatswood, NSW, Australia S K Webber M A Lawless G L Sutton C M Rogers Correspondence to: Dr Michael Lawless, Level 3, 7 Victoria Avenue, Chatswood,
The Short Term Effects of a Single Limbal Relaxing Incision Combined with Clear Corneal Incision
 pissn: 1011-8942 eissn: 2092-9382 Korean J Ophthalmol 2010;24(2):78-82 DOI: 10.3341/kjo.2010.24.2.78 Original Article The Short Term Effects of a Single Limbal Relaxing Incision Combined with Clear Corneal
pissn: 1011-8942 eissn: 2092-9382 Korean J Ophthalmol 2010;24(2):78-82 DOI: 10.3341/kjo.2010.24.2.78 Original Article The Short Term Effects of a Single Limbal Relaxing Incision Combined with Clear Corneal
AXsys Studay Data and Press Release Reference
 Clinically Tested to be the World s Most Accurate Toric Marking Device AXsys Studay Data and Press Release Reference Press Release Reference electronic leveling device for implantation of a toric iol The
Clinically Tested to be the World s Most Accurate Toric Marking Device AXsys Studay Data and Press Release Reference Press Release Reference electronic leveling device for implantation of a toric iol The
Toric intraocular lenses
 Supplement to EyeWorld August 2015 Driving adoption and outcomes with toric IOLs: Pre-, intra-, and postoperative pearls for success 2014 ASCRS Clinical Survey: Trends in toric IOL implementation Click
Supplement to EyeWorld August 2015 Driving adoption and outcomes with toric IOLs: Pre-, intra-, and postoperative pearls for success 2014 ASCRS Clinical Survey: Trends in toric IOL implementation Click
4/9/2016. Sources of. Single-angle vs. double-angle plots for astigmatism data. Commercial Toric IOL calculators. Unexpected residual astigmatism!
 Sources of Corneal astigmatism measurements Methods of calculation Corneal surgically induced astigmatism (SIA) Toric IOL misalignment Unexpected residual astigmatism! Single-angle vs. double-angle plots
Sources of Corneal astigmatism measurements Methods of calculation Corneal surgically induced astigmatism (SIA) Toric IOL misalignment Unexpected residual astigmatism! Single-angle vs. double-angle plots
Irregular Corneal Astigmatism & Cataract
 Costas Karabatsas MD, PhD, MRCOphth, FEBOphth, FRCS Ophth Irregular Corneal Astigmatism & Cataract (assessing ocular surface, IOL selection) In both LRS and Cataract Surgery aim = Emmetropia Refractive
Costas Karabatsas MD, PhD, MRCOphth, FEBOphth, FRCS Ophth Irregular Corneal Astigmatism & Cataract (assessing ocular surface, IOL selection) In both LRS and Cataract Surgery aim = Emmetropia Refractive
Index. D DALK, 69, 155 Differential sector index (DSI), 92 Discriminant function analysis, DMEK, 23 Donor factors, 156 DSAEK, 23
, 92 Discriminant function analysis, DMEK, 23 Donor factors, 156 DSAEK, 23") A Abberrometry, intraoperative, 66 Aberrated corneas, topography-guided laser for, 146 Aberration coefficient, 99 corneal, 94 Ablation cylindrical, 131 hyperopic, 130, 131 pattern, design and planning,
A Abberrometry, intraoperative, 66 Aberrated corneas, topography-guided laser for, 146 Aberration coefficient, 99 corneal, 94 Ablation cylindrical, 131 hyperopic, 130, 131 pattern, design and planning,
Arcuate Keratotomy for High Postoperative Keratoplasty Astigmatism Performed With the IntraLase Femtosecond Laser
 Arcuate Keratotomy for High Postoperative Keratoplasty Astigmatism Performed With the IntraLase Femtosecond Laser Luca Buzzonetti, MD; Gianni Petrocelli, MD; Antonio Laborante, MD; Emilio Mazzilli, MD;
Arcuate Keratotomy for High Postoperative Keratoplasty Astigmatism Performed With the IntraLase Femtosecond Laser Luca Buzzonetti, MD; Gianni Petrocelli, MD; Antonio Laborante, MD; Emilio Mazzilli, MD;
White Paper. Astigmatism Management With Toric IOLs The Importance of Rotational Stability After IOL Implantation. Xiaolin Gu, M.D., PhD.
 White Paper Astigmatism Management With Toric IOLs The Importance of Rotational Stability After IOL Implantation Xiaolin Gu, M.D., PhD. Introduction Cataracts, or clouding of the crystalline lens, are
White Paper Astigmatism Management With Toric IOLs The Importance of Rotational Stability After IOL Implantation Xiaolin Gu, M.D., PhD. Introduction Cataracts, or clouding of the crystalline lens, are
Total corneal astigmatism in older adults taking into account posterior corneal astigmatism by ray tracing
 ARTICLE Total corneal astigmatism in older adults taking into account posterior corneal astigmatism by ray tracing Alvaro Rodríguez Ratón, MD 1 ; Javier Orbegozo Gárate, MD 1 ; Iñaki Basterra Barrenetxea,OD
ARTICLE Total corneal astigmatism in older adults taking into account posterior corneal astigmatism by ray tracing Alvaro Rodríguez Ratón, MD 1 ; Javier Orbegozo Gárate, MD 1 ; Iñaki Basterra Barrenetxea,OD
Premium treatment starts with premium diagnosis
 by i-optics Premium treatment starts with premium diagnosis Complete your cataract-refractive platform The premium IOL opportunity Premium IOL market to nearly double in next 5 years 2013 1.6 million 22
by i-optics Premium treatment starts with premium diagnosis Complete your cataract-refractive platform The premium IOL opportunity Premium IOL market to nearly double in next 5 years 2013 1.6 million 22
Management of astigmatism at the time of cataract or refractive lens surgery has evolved to include arcuate keratotomy and toric
 Management of Astigmatism with the LENSAR Laser System with Streamline Mark Packer Mark Packer MD Consulting, Inc., Boulder, CO, US DOI: https://doi.org/10.17925/usor.2017.12.99 Management of astigmatism
Management of Astigmatism with the LENSAR Laser System with Streamline Mark Packer Mark Packer MD Consulting, Inc., Boulder, CO, US DOI: https://doi.org/10.17925/usor.2017.12.99 Management of astigmatism
No financial interest
 Management of high astigmatism after penetrating keratoplasty Ahmed Sherif MD Assistant Professor of Ophthalmology Cairo University No financial interest 1 Incidence Several reports state that 15-31% of
Management of high astigmatism after penetrating keratoplasty Ahmed Sherif MD Assistant Professor of Ophthalmology Cairo University No financial interest 1 Incidence Several reports state that 15-31% of
Douglas Katsev MD Sansum Clinic Chairman Ophthalmology Santa Barbara CA
 Early Outcomes (9 months) with a Toric Accommodating IOL How do They Fit in My refractive Practice Douglas Katsev MD Sansum Clinic i Chairman Ophthalmology Santa Barbara CA 1 Disclosure Consulting Fee:
Early Outcomes (9 months) with a Toric Accommodating IOL How do They Fit in My refractive Practice Douglas Katsev MD Sansum Clinic i Chairman Ophthalmology Santa Barbara CA 1 Disclosure Consulting Fee:
Femtosecond Cataract Surgery: Correction of Astigmatism and Complex Cases Financial Disclosures Femtosecond Laser Utility in Cataract Surgery
 1 2 3 4 5 6 7 Femtosecond Cataract Surgery: Correction of Astigmatism and Complex Cases Michael J Taravella, MD Director: Cornea and Refractive Surgery University of Colorado Financial Disclosures Consultant
1 2 3 4 5 6 7 Femtosecond Cataract Surgery: Correction of Astigmatism and Complex Cases Michael J Taravella, MD Director: Cornea and Refractive Surgery University of Colorado Financial Disclosures Consultant
Arthur Cummings FRCSEd
 How to Improve your Refractive Cataract Surgery Outcomes by Skilful Interpretation of Corneal Mapping Course IC-16 ESCRS Copenhagen 10 th September 2016 Consultant for Alcon / WaveLight/TearLab Arthur
How to Improve your Refractive Cataract Surgery Outcomes by Skilful Interpretation of Corneal Mapping Course IC-16 ESCRS Copenhagen 10 th September 2016 Consultant for Alcon / WaveLight/TearLab Arthur
POST-OPERATIVE ASTIGMATISM AFTER SICS AND PHACOEMULSIFICATION.
 4 POST-OPERATIVE ASTIGMATISM AFTER SICS AND PHACOEMULSIFICATION. Dr.Vijay Damor, Dr.Anupama Mahant, Department of ophthalmology,amc MET Medical college. Ahmedabad pin 380008 Abstract : Background: Astigmatism
4 POST-OPERATIVE ASTIGMATISM AFTER SICS AND PHACOEMULSIFICATION. Dr.Vijay Damor, Dr.Anupama Mahant, Department of ophthalmology,amc MET Medical college. Ahmedabad pin 380008 Abstract : Background: Astigmatism
Predicting of Uncorrected Astigmatism from Decimal Visual Acuity in Spherical Equivalent
 Journal of the Optical Society of Korea Vol. 17, No. 2, April 2013, pp. 219-223 DOI: http://dx.doi.org/10.3807/josk.2013.17.2.219 Predicting of Uncorrected Astigmatism from Decimal Visual Acuity in Spherical
Journal of the Optical Society of Korea Vol. 17, No. 2, April 2013, pp. 219-223 DOI: http://dx.doi.org/10.3807/josk.2013.17.2.219 Predicting of Uncorrected Astigmatism from Decimal Visual Acuity in Spherical
2Optimizing the Refractive
 Chapter 02 3/4/11 4:29 PM Page 1 2Optimizing the Refractive Outcome: Correction of Astigmatism in Cataract Surgery By: Robert M. Kershner, M.D., FACS General Considerations Lens extraction with the implantation
Chapter 02 3/4/11 4:29 PM Page 1 2Optimizing the Refractive Outcome: Correction of Astigmatism in Cataract Surgery By: Robert M. Kershner, M.D., FACS General Considerations Lens extraction with the implantation
Full-Thickness Astigmatic Keratotomy Combined With Small-Incision Lenticule Extraction to Treat High-Level and Mixed Astigmatism
 CLINICAL SCIENCE Full-Thickness Astigmatic Keratotomy Combined With Small-Incision Lenticule Extraction to Treat High-Level and Mixed Astigmatism Bu Ki Kim, MD, MS,* Su Joung Mun, MD, PhD,* Dae Gyu Lee,
CLINICAL SCIENCE Full-Thickness Astigmatic Keratotomy Combined With Small-Incision Lenticule Extraction to Treat High-Level and Mixed Astigmatism Bu Ki Kim, MD, MS,* Su Joung Mun, MD, PhD,* Dae Gyu Lee,
Richard N. McNeely 1,2, Salissou Moutari 3, Eric Pazo 1,2 and Jonathan E. Moore 1,2*
 McNeely et al. Eye and Vision (2018) 5:7 https://doi.org/10.1186/s40662-018-0103-4 RESEARCH Investigating the impact of preoperative corneal astigmatism orientation on the postoperative spherical equivalent
McNeely et al. Eye and Vision (2018) 5:7 https://doi.org/10.1186/s40662-018-0103-4 RESEARCH Investigating the impact of preoperative corneal astigmatism orientation on the postoperative spherical equivalent
Evaluation of Opposite Clear Corneal Incision in Controlling Astigmatism in Cataract Patients Undergoing Phacoemulsification Surgery
 Evaluation of Opposite Clear Corneal Incision in Controlling Astigmatism in Cataract Patients Undergoing Phacoemulsification Surgery J.S.Bhalla, Meenakshi Rani, Surbhi Gupta Department of Ophthalmology,
Evaluation of Opposite Clear Corneal Incision in Controlling Astigmatism in Cataract Patients Undergoing Phacoemulsification Surgery J.S.Bhalla, Meenakshi Rani, Surbhi Gupta Department of Ophthalmology,
AXsys Study Data and Press Release Reference
 Clinically Tested to be the World s Most Accurate Toric Marking Device Takayuki Akahoshi, MD Tokyo Japan Ophthalmologist Anterior Segment I WORKED WITH ASICO LLC TO DESIGN AN AXsys TM TORIC MARKING DEVICE
Clinically Tested to be the World s Most Accurate Toric Marking Device Takayuki Akahoshi, MD Tokyo Japan Ophthalmologist Anterior Segment I WORKED WITH ASICO LLC TO DESIGN AN AXsys TM TORIC MARKING DEVICE
Circular Keratotomy to Reduce Astigmatism and Improve Vision in Stage I and II Keratoconus
 Circular Keratotomy to Reduce Astigmatism and Improve Vision in Stage I and II Keratoconus Jorg H. Krumeich, MD; Guy M. Kezirian, MD, FACS ABSTRACT PURPOSE: To report the use of circular keratotomy in
Circular Keratotomy to Reduce Astigmatism and Improve Vision in Stage I and II Keratoconus Jorg H. Krumeich, MD; Guy M. Kezirian, MD, FACS ABSTRACT PURPOSE: To report the use of circular keratotomy in
Phacoemulsification: The first 50 Cases
 Phacoemulsification: The first 5 Cases Aneeq Ullah Baig Mirza*, Samina Jehangir**, Wasif Mohy-ud-din Kadri** * Department of Ophthalmology Islamic International Medical College and Railway Hospital Rawalpindi.
Phacoemulsification: The first 5 Cases Aneeq Ullah Baig Mirza*, Samina Jehangir**, Wasif Mohy-ud-din Kadri** * Department of Ophthalmology Islamic International Medical College and Railway Hospital Rawalpindi.
Handout Course Title : Astigmatisme Management with toric IOL
 Handout Course Title : Astigmatisme Management with toric IOL ESCRS Milano 2012 Level :Basic Course leader : Jerome jean Bovet Course duration : 2 hours Faculty : Jerome Bovet, Warren Hill Keiki Mehta
Handout Course Title : Astigmatisme Management with toric IOL ESCRS Milano 2012 Level :Basic Course leader : Jerome jean Bovet Course duration : 2 hours Faculty : Jerome Bovet, Warren Hill Keiki Mehta
2nd ESASO Anterior Segment Academy April 2016, Milano/Italy
 2nd ESASO Anterior 28 30 April 2016, Milano/Italy Istituto Clinico Humanitas Humanitas Congress Centre Via Manzoni, 56 20089 Rozzano, Milan Congress Chairmen: José L. Güell, Paolo Vinciguerra www.esaso.org/2nd-esaso-anteriorsegment-academy-2016/
2nd ESASO Anterior 28 30 April 2016, Milano/Italy Istituto Clinico Humanitas Humanitas Congress Centre Via Manzoni, 56 20089 Rozzano, Milan Congress Chairmen: José L. Güell, Paolo Vinciguerra www.esaso.org/2nd-esaso-anteriorsegment-academy-2016/
Prospective study of toric IOL outcomes based on the Lenstar LS 900 W dual zone automated keratometer
 Gundersen and Potvin BMC Ophthalmology 2012, 12:21 RESEARCH ARTICLE Open Access Prospective study of toric IOL outcomes based on the Lenstar LS 900 W dual zone automated keratometer Kjell Gunnar Gundersen
Gundersen and Potvin BMC Ophthalmology 2012, 12:21 RESEARCH ARTICLE Open Access Prospective study of toric IOL outcomes based on the Lenstar LS 900 W dual zone automated keratometer Kjell Gunnar Gundersen
Comparison of the Astigmatic Power of Toric Intraocular Lenses Using Three Toric Calculators
 Original Article http://dx.doi.org/10.3349/ymj.2015.56.4.1097 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 56(4):1097-1105, 2015 Comparison of the Astigmatic Power of Toric Intraocular Lenses Using
Original Article http://dx.doi.org/10.3349/ymj.2015.56.4.1097 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 56(4):1097-1105, 2015 Comparison of the Astigmatic Power of Toric Intraocular Lenses Using
New method of quantifying corneal topographic astigmatism that corresponds with manifest refractive cylinder
 ARTICLE New method of quantifying corneal topographic astigmatism that corresponds with manifest refractive cylinder Noel Alpins, FRANZCO, FRCOphth, FACS, James K.Y. Ong, BOptom, Dr.rer.nat, George Stamatelatos,
ARTICLE New method of quantifying corneal topographic astigmatism that corresponds with manifest refractive cylinder Noel Alpins, FRANZCO, FRCOphth, FACS, James K.Y. Ong, BOptom, Dr.rer.nat, George Stamatelatos,
Clinical Study Effect of Pupil Size on Optical Quality Parameters in Astigmatic Eyes Using a Double-Pass Instrument
 BioMed Research International Volume 2013, Article ID 124327, 6 pages http://dx.doi.org/1155/2013/124327 Clinical Study Effect of Pupil Size on Optical Quality Parameters in Astigmatic Eyes Using a Double-Pass
BioMed Research International Volume 2013, Article ID 124327, 6 pages http://dx.doi.org/1155/2013/124327 Clinical Study Effect of Pupil Size on Optical Quality Parameters in Astigmatic Eyes Using a Double-Pass
Development of a program for toric intraocular lens calculation. considering posterior corneal astigmatism, incisioninduced
 DOI 10.1007/s00417-016-3446-3 CATARACT Development of a program for toric intraocular lens calculation considering posterior corneal astigmatism, incision-induced posterior corneal astigmatism, and effective
DOI 10.1007/s00417-016-3446-3 CATARACT Development of a program for toric intraocular lens calculation considering posterior corneal astigmatism, incision-induced posterior corneal astigmatism, and effective
Clinical results of arcuate incisions to correct astigmatism
 Clinical results of arcuate incisions to correct astigmatism Kurt A. Buzard, MD, Eduardo Laranjeira, MD, Bradley R. Fundingsland, BS ABSTRACT Purpose: To evaluate the effectiveness of arcuate incisions
Clinical results of arcuate incisions to correct astigmatism Kurt A. Buzard, MD, Eduardo Laranjeira, MD, Bradley R. Fundingsland, BS ABSTRACT Purpose: To evaluate the effectiveness of arcuate incisions
Postoperative Astigmatic Outcomes Based on the Haptic Axis of Intraocular Lenses Inserted in Cataract Surgery
 pissn: 1011-8942 eissn: 2092-9382 Korean J Ophthalmol 2011;25(1):22-28 DOI: 10.3341/kjo.2011.25.1.22 Original Article Postoperative Astigmatic Outcomes Based on the Haptic Axis of Intraocular Lenses Inserted
pissn: 1011-8942 eissn: 2092-9382 Korean J Ophthalmol 2011;25(1):22-28 DOI: 10.3341/kjo.2011.25.1.22 Original Article Postoperative Astigmatic Outcomes Based on the Haptic Axis of Intraocular Lenses Inserted
CHANGE ON THE HORIZONTAL AND VERTICAL MERIDIANS OF THE CORNEA AFTER CATARACT SURGERY*
 15 Merriam Final 11/9/01 11:22 AM Page 187 CHANGE ON THE HORIZONTAL AND VERTICAL MERIDIANS OF THE CORNEA AFTER CATARACT SURGERY* BY John C. Merriam, MD, Lei Zheng, MD (BY INVITATION), Joanna Urbanowicz,
15 Merriam Final 11/9/01 11:22 AM Page 187 CHANGE ON THE HORIZONTAL AND VERTICAL MERIDIANS OF THE CORNEA AFTER CATARACT SURGERY* BY John C. Merriam, MD, Lei Zheng, MD (BY INVITATION), Joanna Urbanowicz,
THE CHALLENGES CORNEAL IRREGULARITIES POST-LASIK ECTASIA IS THIS A GOOD LASIK CANDIDATE? 3/5/2015. FITTING THE IRREGULAR CORNEA Challenges & Solutions
 DISCLOSURE STATEMENT No disclosure statement. CORNEAL IRREGULARITIES Course Title: Lecturer: FITTING THE IRREGULAR CORNEA Challenges & Solutions Phyllis Rakow, COMT, NCLM, FCLSA(H) Keratoconus Pseudokeratoconus
DISCLOSURE STATEMENT No disclosure statement. CORNEAL IRREGULARITIES Course Title: Lecturer: FITTING THE IRREGULAR CORNEA Challenges & Solutions Phyllis Rakow, COMT, NCLM, FCLSA(H) Keratoconus Pseudokeratoconus
Over the last decade, a vast improvement on intraocular
 REVIEW Posterior Astigmatism: Considerations for Cataract Refractive Surgery Planning Milton S. Yogi, MD, MBA1 Bruna V. Ventura, MD, PhD2 Eliane M. Nakano, MD3 1 Head, Cataract Department, Beneficência
REVIEW Posterior Astigmatism: Considerations for Cataract Refractive Surgery Planning Milton S. Yogi, MD, MBA1 Bruna V. Ventura, MD, PhD2 Eliane M. Nakano, MD3 1 Head, Cataract Department, Beneficência
STUDY OF ASTIGMATISM IN SMALL INCISSION CATARACT SURGERY BETWEEN TEMPORAL AND SUPERIOR INCISSIONS K. J. N. Sivacharan 1, G.
 STUDY OF ASTIGMATISM IN SMALL INCISSION CATARACT SURGERY BETWEEN TEMPORAL AND SUPERIOR INCISSIONS K. J. N. Sivacharan 1, G. Hanumantharao 2 HOW TO CITE THIS ARTICLE: K. J. N. Sivacharan, G. Hanumantharao.
STUDY OF ASTIGMATISM IN SMALL INCISSION CATARACT SURGERY BETWEEN TEMPORAL AND SUPERIOR INCISSIONS K. J. N. Sivacharan 1, G. Hanumantharao 2 HOW TO CITE THIS ARTICLE: K. J. N. Sivacharan, G. Hanumantharao.
Assessment & management of irregular astigmatism
 Assessment & management of irregular astigmatism Athens, March 2018 D. Epstein, MD, PhD, FARVO No financial interest What is an irregular astigmatism? A question that starts at the wrong end... How about
Assessment & management of irregular astigmatism Athens, March 2018 D. Epstein, MD, PhD, FARVO No financial interest What is an irregular astigmatism? A question that starts at the wrong end... How about
Comparison of Toric Foldable Iris-Fixated Phakic Intraocular Lens Implantation and Limbal Relaxing Incisions for Moderate-to-High Myopic Astigmatism
 Original Article Yonsei Med J 216 Nov;57(6):1475-1481 pissn: 513-5796 eissn: 1976-2437 Comparison of Toric Foldable Iris-Fixated Phakic Intraocular Lens Implantation and Limbal Relaxing Incisions for Moderate-to-High
Original Article Yonsei Med J 216 Nov;57(6):1475-1481 pissn: 513-5796 eissn: 1976-2437 Comparison of Toric Foldable Iris-Fixated Phakic Intraocular Lens Implantation and Limbal Relaxing Incisions for Moderate-to-High
The efficacy of Toric IOL in comparison to LRI in correcting pre-existing astigmatism in phacoemulsification
 Original Research Article The efficacy of Toric IOL in comparison to LRI in correcting pre-existing astigmatism in phacoemulsification Parul Singh 1, Ruchika Agarwal 2*, Sanjeev Rohatgi 2, Malini Vohra
Original Research Article The efficacy of Toric IOL in comparison to LRI in correcting pre-existing astigmatism in phacoemulsification Parul Singh 1, Ruchika Agarwal 2*, Sanjeev Rohatgi 2, Malini Vohra
A novel method for human Astigmatism formulation and measurement
 Available online at http://www.ijabbr.com International journal of Advanced Biological and Biomedical Research Volume 1, Issue 8, 2013: 874-884 A novel method for human Astigmatism formulation and measurement
Available online at http://www.ijabbr.com International journal of Advanced Biological and Biomedical Research Volume 1, Issue 8, 2013: 874-884 A novel method for human Astigmatism formulation and measurement
Effect of Pupil Size on Uncorrected Visual Acuity in Pseudophakic Eyes With Astigmatism
 ORIGINAL ARTICLE Effect of Pupil Size on Uncorrected Visual Acuity in Pseudophakic Eyes With Astigmatism Kazuhiro Watanabe, MD; Kazuno Negishi, MD; Murat Dogru, MD; Takefumi Yamaguchi, MD; Hidemasa Torii,
ORIGINAL ARTICLE Effect of Pupil Size on Uncorrected Visual Acuity in Pseudophakic Eyes With Astigmatism Kazuhiro Watanabe, MD; Kazuno Negishi, MD; Murat Dogru, MD; Takefumi Yamaguchi, MD; Hidemasa Torii,
Handheld Shack Hartmann Wavefront Sensor. Jim Schwiegerling, Ph.D. Department of Ophthalmology and Optical Sciences The University of Arizona
 Handheld Shack Hartmann Wavefront Sensor Jim Schwiegerling, Ph.D. Department of Ophthalmology and Optical Sciences The University of Arizona COLLABORATORS Erin M. Harvey, PhD Velma Dobson, PhD Joseph M.
Handheld Shack Hartmann Wavefront Sensor Jim Schwiegerling, Ph.D. Department of Ophthalmology and Optical Sciences The University of Arizona COLLABORATORS Erin M. Harvey, PhD Velma Dobson, PhD Joseph M.
Irregular Astigmatism Diagnosis And Treatment
 Irregular Astigmatism Diagnosis And Treatment 1 / 5 2 / 5 3 / 5 Irregular Astigmatism Diagnosis And Treatment Irregular Astigmatism: Diagnosis and Treatment. Ming Wang, ed., Thorofare, NJ: Slack Inc.;
Irregular Astigmatism Diagnosis And Treatment 1 / 5 2 / 5 3 / 5 Irregular Astigmatism Diagnosis And Treatment Irregular Astigmatism: Diagnosis and Treatment. Ming Wang, ed., Thorofare, NJ: Slack Inc.;
CA-800 Tear Module. Rick Gaudenti. Product Manager, Refraction Mar 2017
 CA-800 Tear Module Rick Gaudenti Product Manager, Refraction Mar 2017 Meibomian Gland Imaging Meibomian Gland [MEIB] Viewing Meibomian Images are displayed in the center of the screen Two types of an adjustable
CA-800 Tear Module Rick Gaudenti Product Manager, Refraction Mar 2017 Meibomian Gland Imaging Meibomian Gland [MEIB] Viewing Meibomian Images are displayed in the center of the screen Two types of an adjustable
Perioperative Modulating Factors on Astigmatism in Sutured Cataract Surgery
 접수번호 : 2008-114 Korean Journal of Ophthalmology 2009;23:240-248 ISSN : 1011-8942 DOI : 10.3341/kjo.2009.23.4.240 Perioperative Modulating Factors on Astigmatism in Sutured Cataract Surgery Yang Kyeung
접수번호 : 2008-114 Korean Journal of Ophthalmology 2009;23:240-248 ISSN : 1011-8942 DOI : 10.3341/kjo.2009.23.4.240 Perioperative Modulating Factors on Astigmatism in Sutured Cataract Surgery Yang Kyeung
Orthokeratology (Ortho-K), or corneal refractive therapy, is. Toric Double Tear Reservoir Contact Lens in Orthokeratology for Astigmatism ARTICLE
, or corneal refractive therapy, is. Toric Double Tear Reservoir Contact Lens in Orthokeratology for Astigmatism ARTICLE") ARTICLE Toric Double Tear Reservoir Contact Lens in Orthokeratology for Astigmatism Jaume Pauné, M.Sc., Genís Cardona, Ph.D., and Lluïsa Quevedo, Ph.D. Objectives: This study aimed at assessing the performance
ARTICLE Toric Double Tear Reservoir Contact Lens in Orthokeratology for Astigmatism Jaume Pauné, M.Sc., Genís Cardona, Ph.D., and Lluïsa Quevedo, Ph.D. Objectives: This study aimed at assessing the performance
Multicolor Scan Laser Photocoagulator MC-500 Vixi
 Multicolor Scan Laser Photocoagulator MC-500 Vixi MC-500 The Versatile Laser Photocoagulator Selectable configuration of laser colors and delivery units Multiple scan patterns Enhanced usability LPM (Low
Multicolor Scan Laser Photocoagulator MC-500 Vixi MC-500 The Versatile Laser Photocoagulator Selectable configuration of laser colors and delivery units Multiple scan patterns Enhanced usability LPM (Low
Femtosecond laser-assisted astigmatic keratotomy: a review
 Chang Eye and Vision (2018) 5:6 https://doi.org/10.1186/s40662-018-0099-9 REVIEW Open Access Femtosecond laser-assisted astigmatic keratotomy: a review John S. M. Chang Abstract Background: Astigmatic
Chang Eye and Vision (2018) 5:6 https://doi.org/10.1186/s40662-018-0099-9 REVIEW Open Access Femtosecond laser-assisted astigmatic keratotomy: a review John S. M. Chang Abstract Background: Astigmatic
Astigmatism in Children: Changes in Axis and Amount from Birth to Six Years
 Astigmatism in Children: Changes in Axis and Amount from Birth to Six Years Jane Gwiazda, Mitchell Scheiman,* Indra Mohindra, and Richard Held Noncycloplegic refractions of, children aged - years revealed
Astigmatism in Children: Changes in Axis and Amount from Birth to Six Years Jane Gwiazda, Mitchell Scheiman,* Indra Mohindra, and Richard Held Noncycloplegic refractions of, children aged - years revealed
Research conducted over the past 15 years has yielded a
 Visual Psychophysics and Physiological Optics Longitudinal Change and Stability of Refractive, Keratometric, and Internal Astigmatism in Childhood Erin M. Harvey, 1,2 Joseph M. Miller, 1 3 J. Daniel Twelker,
Visual Psychophysics and Physiological Optics Longitudinal Change and Stability of Refractive, Keratometric, and Internal Astigmatism in Childhood Erin M. Harvey, 1,2 Joseph M. Miller, 1 3 J. Daniel Twelker,
Dr Noel Alpins AM Digest of Personal and Professional biography
 Dr Noel Alpins AM Digest of Personal and Professional biography Work Address: 7 Chesterville Road Cheltenham 3192 Dr Noel Alpins AM has been specialising in Cataract and Refractive Surgery since founding
Dr Noel Alpins AM Digest of Personal and Professional biography Work Address: 7 Chesterville Road Cheltenham 3192 Dr Noel Alpins AM has been specialising in Cataract and Refractive Surgery since founding
AstigmatismamongotherRefractiveErrorsinChildrenofSouthernSriLanka. Astigmatism among other Refractive Errors in Children of Southern Sri Lanka
 : F Diseases Volume 15 Issue 1 Version 1.0 Year 2015 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Inc. (USA) Online ISSN: 2249-4618 & Print ISSN: 0975-5888
: F Diseases Volume 15 Issue 1 Version 1.0 Year 2015 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Inc. (USA) Online ISSN: 2249-4618 & Print ISSN: 0975-5888
1. Standard Equipment Subjective Eye Tester Name of Parts Details of Auxiliary Lenses Measuring Performance...
 Notification Dear Users, Thank you for your purchase of R 2500 Refractor. Please take time to read our user s manual carefully before use. This guarantees you to make full use of this unit and prolongs
Notification Dear Users, Thank you for your purchase of R 2500 Refractor. Please take time to read our user s manual carefully before use. This guarantees you to make full use of this unit and prolongs
OPTOMETRY. An analysis of the astigmatic changes induced by accelerated o rt ho ke ratolog y I ORIGINALPAPER 1
 OPTOMETRY I ORIGINALPAPER 1 An analysis of the astigmatic changes induced by accelerated o rt ho ke ratolog y Clin Exp Optom ; 85: 5: 84-93 John Mountford* DipAppSc FAAO FVCO FCLS Konrad Pesudovst PhD
OPTOMETRY I ORIGINALPAPER 1 An analysis of the astigmatic changes induced by accelerated o rt ho ke ratolog y Clin Exp Optom ; 85: 5: 84-93 John Mountford* DipAppSc FAAO FVCO FCLS Konrad Pesudovst PhD
Eyes with regular astigmatism have two orthogonal focal. Accommodation in Astigmatic Children During Visual Task Performance
 Clinical and Epidemiologic Research Accommodation in Astigmatic Children During Visual Task Performance Erin M. Harvey, 1,2 Joseph M. Miller, 1 3 Howard P. Apple, 1 Pavan Parashar, 4 J. Daniel Twelker,
Clinical and Epidemiologic Research Accommodation in Astigmatic Children During Visual Task Performance Erin M. Harvey, 1,2 Joseph M. Miller, 1 3 Howard P. Apple, 1 Pavan Parashar, 4 J. Daniel Twelker,
Analysis of WFS Measurements from first half of 2004
 Analysis of WFS Measurements from first half of 24 (Report4) Graham Cox August 19, 24 1 Abstract Described in this report is the results of wavefront sensor measurements taken during the first seven months
Analysis of WFS Measurements from first half of 24 (Report4) Graham Cox August 19, 24 1 Abstract Described in this report is the results of wavefront sensor measurements taken during the first seven months
Astigmatic axis and amblyopia in childhood
 Astigmatic axis and amblyopia in childhood Maths Abrahamsson and Johan Sjo strand ABSTRACT. Purpose: This study is part of a larger project whose aim is to evaluate the relationship between refractive
Astigmatic axis and amblyopia in childhood Maths Abrahamsson and Johan Sjo strand ABSTRACT. Purpose: This study is part of a larger project whose aim is to evaluate the relationship between refractive
Cycloplegic Refractions of Infants and Young Children: The Axis of Astigmatism
 Cycloplegic Refractions of Infants and Young Children: The Axis of Astigmatism Velma Dobson,* Anne B. Fulton, f and S. Lawson Sebris* Review of the cycloplegic refractions of all children who were first
Cycloplegic Refractions of Infants and Young Children: The Axis of Astigmatism Velma Dobson,* Anne B. Fulton, f and S. Lawson Sebris* Review of the cycloplegic refractions of all children who were first
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
A R Sebai Sarhan, Harminder S Dua, Michelle Beach
 Br J Ophthalmol 2000;84:837 841 837 Division of Ophthalmology and Visual Sciences, University of Nottingham, University Hospital, Queen s Medical Centre, Nottingham NG7 2UH A R S Sarhan H S Dua M Beach
Br J Ophthalmol 2000;84:837 841 837 Division of Ophthalmology and Visual Sciences, University of Nottingham, University Hospital, Queen s Medical Centre, Nottingham NG7 2UH A R S Sarhan H S Dua M Beach
MC-500 Vixi MC-500. Multicolor Scan Laser Photocoagulator. Multicolor Laser Photocoagulator US EDITION
 Multicolor Scan Laser Photocoagulator MC-500 Vixi MC-500 Multicolor Laser Photocoagulator US EDITION MC-500 / MC-500 The Versatile Laser Photocoagulator The versatility of the MC-500 Vixi / MC-500 speaks
Multicolor Scan Laser Photocoagulator MC-500 Vixi MC-500 Multicolor Laser Photocoagulator US EDITION MC-500 / MC-500 The Versatile Laser Photocoagulator The versatility of the MC-500 Vixi / MC-500 speaks
620 Rejwrts Investigative Ophthalmology
 Rejwrts Investigative Ophthalmology August D. E.: Retinal dystrophy in the rat a pigment epithelial disease, INVEST. OPHTHALMOL. :,. Color vision: blue deficiencies in? ANTHONY J. ADAMS,* RICHARD BAL-
Rejwrts Investigative Ophthalmology August D. E.: Retinal dystrophy in the rat a pigment epithelial disease, INVEST. OPHTHALMOL. :,. Color vision: blue deficiencies in? ANTHONY J. ADAMS,* RICHARD BAL-
ORIGINAL ARTICLE. Amblyopia in Astigmatic Infants and Toddlers
 1040-5488/10/8705-0330/0 VOL. 87, NO. 5, PP. 330 336 OPTOMETRY AND VISION SCIENCE Copyright 2010 American Academy of Optometry ORIGINAL ARTICLE Amblyopia in Astigmatic Infants and Toddlers Velma Dobson*,
1040-5488/10/8705-0330/0 VOL. 87, NO. 5, PP. 330 336 OPTOMETRY AND VISION SCIENCE Copyright 2010 American Academy of Optometry ORIGINAL ARTICLE Amblyopia in Astigmatic Infants and Toddlers Velma Dobson*,
Diagnosis and Management of Astigmatism
 Diagnosis and Management of Astigmatism Ray George Diagnosis and Management of Astigmatism "This page is Intentionally Left Blank" Diagnosis and Management of Astigmatism Edited by Ray George Published
Diagnosis and Management of Astigmatism Ray George Diagnosis and Management of Astigmatism "This page is Intentionally Left Blank" Diagnosis and Management of Astigmatism Edited by Ray George Published
ORIGINAL ARTICLE. Corneal and Refractive Error Astigmatism in Singaporean Schoolchildren: a Vector-Based Javal s Rule
 1040-5488/01/7812-0881/0 VOL. 78, NO. 12, PP. 881 887 OPTOMETRY AND VISION SCIENCE Copyright 2001 American Academy of Optometry ORIGINAL ARTICLE Corneal and Refractive Error Astigmatism in Singaporean
1040-5488/01/7812-0881/0 VOL. 78, NO. 12, PP. 881 887 OPTOMETRY AND VISION SCIENCE Copyright 2001 American Academy of Optometry ORIGINAL ARTICLE Corneal and Refractive Error Astigmatism in Singaporean
Refractive, anterior corneal and internal astigmatism in the pseudophakic eye
 Refractive, anterior corneal and internal astigmatism in the pseudophakic eye Jesper F. Bregnhøj, 1,2 Pourang Mataji 1,2 and Kristian Næser 1,2 1 Department of Ophthalmology, Aarhus University Hospital,
Refractive, anterior corneal and internal astigmatism in the pseudophakic eye Jesper F. Bregnhøj, 1,2 Pourang Mataji 1,2 and Kristian Næser 1,2 1 Department of Ophthalmology, Aarhus University Hospital,
Correcting Your Vision: Advice and Opinions from an Eye Surgeon Health Radio April 17, 2007 Mark Walker, M.D. Introduction
 Correcting Your Vision: Advice and Opinions from an Eye Surgeon Health Radio April 17, 2007 Mark Walker, M.D. Please remember the opinions expressed on Patient Power are not necessarily the views of Health
Correcting Your Vision: Advice and Opinions from an Eye Surgeon Health Radio April 17, 2007 Mark Walker, M.D. Please remember the opinions expressed on Patient Power are not necessarily the views of Health
Comparison of Mixed-Effects Model, Pattern-Mixture Model, and Selection Model in Estimating Treatment Effect Using PRO Data in Clinical Trials
 Comparison of Mixed-Effects Model, Pattern-Mixture Model, and Selection Model in Estimating Treatment Effect Using PRO Data in Clinical Trials Xiaolei Zhou, 1,2 Jianmin Wang, 1 Jessica Zhang, 1 Hongtu
Comparison of Mixed-Effects Model, Pattern-Mixture Model, and Selection Model in Estimating Treatment Effect Using PRO Data in Clinical Trials Xiaolei Zhou, 1,2 Jianmin Wang, 1 Jessica Zhang, 1 Hongtu
Multicolor Scan Laser Photocoagulator MC-500 Vixi. Multicolor Laser PhotocoagulatorMC-500
 Multicolor Scan Laser Photocoagulator MC-500 Vixi Multicolor Laser PhotocoagulatorMC-500 MC-500 / MC-500 The Versatile Laser Photocoagulator The versatility of the MC-500 Vixi / MC-500 speaks for itself.
Multicolor Scan Laser Photocoagulator MC-500 Vixi Multicolor Laser PhotocoagulatorMC-500 MC-500 / MC-500 The Versatile Laser Photocoagulator The versatility of the MC-500 Vixi / MC-500 speaks for itself.
MODE FIELD DIAMETER AND EFFECTIVE AREA MEASUREMENT OF DISPERSION COMPENSATION OPTICAL DEVICES
 MODE FIELD DIAMETER AND EFFECTIVE AREA MEASUREMENT OF DISPERSION COMPENSATION OPTICAL DEVICES Hale R. Farley, Jeffrey L. Guttman, Razvan Chirita and Carmen D. Pâlsan Photon inc. 6860 Santa Teresa Blvd
MODE FIELD DIAMETER AND EFFECTIVE AREA MEASUREMENT OF DISPERSION COMPENSATION OPTICAL DEVICES Hale R. Farley, Jeffrey L. Guttman, Razvan Chirita and Carmen D. Pâlsan Photon inc. 6860 Santa Teresa Blvd
Proposed classification for topographic patterns seen after penetrating keratoplasty
 Br J Ophthalmol 1999;83:403 409 403 Department of Ophthalmology, Bristol Eye Hospital, Bristol C H Karabatsas S D Cook J M Sparrow Correspondence to: Costas H Karabatsas, PO Box 16757, Athens 115 02, Greece.
Br J Ophthalmol 1999;83:403 409 403 Department of Ophthalmology, Bristol Eye Hospital, Bristol C H Karabatsas S D Cook J M Sparrow Correspondence to: Costas H Karabatsas, PO Box 16757, Athens 115 02, Greece.
NIH Public Access Author Manuscript Optom Vis Sci. Author manuscript; available in PMC 2011 May 1.
 NIH Public Access Author Manuscript Published in final edited form as: Optom Vis Sci. 2010 May ; 87(5): 330 336. doi:10.1097/opx.0b013e3181d951c8. Amblyopia in Astigmatic Infants and Toddlers Velma Dobson,
NIH Public Access Author Manuscript Published in final edited form as: Optom Vis Sci. 2010 May ; 87(5): 330 336. doi:10.1097/opx.0b013e3181d951c8. Amblyopia in Astigmatic Infants and Toddlers Velma Dobson,
How to Chose an Ideal High Definition Endoscopic Camera System
 How to Chose an Ideal High Definition Endoscopic Camera System Telescope Laparoscopy (from Greek lapara, "flank or loin", and skopein, "to see, view or examine") is an operation performed within the abdomen
How to Chose an Ideal High Definition Endoscopic Camera System Telescope Laparoscopy (from Greek lapara, "flank or loin", and skopein, "to see, view or examine") is an operation performed within the abdomen
Most advanced, portable, high-power 532nm Diode-Pumped Solid-State Photocoagulator
 Ophthalmology Since 1970 Most advanced, portable, high-power 532nm Diode-Pumped Solid-State Photocoagulator breakthrough technology FROM A BREAKTHROUGH COMPANY For treatment flexibility, the LaserLink
Ophthalmology Since 1970 Most advanced, portable, high-power 532nm Diode-Pumped Solid-State Photocoagulator breakthrough technology FROM A BREAKTHROUGH COMPANY For treatment flexibility, the LaserLink
Treatment of astigmatism-related amblyopia in 3- to 5-year-old children
 Vision Research 44 (2004) 1623 1634 www.elsevier.com/locate/visres Treatment of astigmatism-related amblyopia in 3- to 5-year-old children Erin M. Harvey a, *, Velma Dobson a,b, Joseph M. Miller a,c,d,
Vision Research 44 (2004) 1623 1634 www.elsevier.com/locate/visres Treatment of astigmatism-related amblyopia in 3- to 5-year-old children Erin M. Harvey a, *, Velma Dobson a,b, Joseph M. Miller a,c,d,
In-process inspection: Inspector technology and concept
 Inspector In-process inspection: Inspector technology and concept Need to inspect a part during production or the final result? The Inspector system provides a quick and efficient method to interface a
Inspector In-process inspection: Inspector technology and concept Need to inspect a part during production or the final result? The Inspector system provides a quick and efficient method to interface a
Litho. Taking care of people, our masterpieces. Surgical Laser System. Surgery
 Taking care of people, our masterpieces Litho Surgical Laser System This brochure is not intended for the U.S. market. Certain Intended Uses/Configurations/Models/Accessories are not cleared for U.S. Surgery
Taking care of people, our masterpieces Litho Surgical Laser System This brochure is not intended for the U.S. market. Certain Intended Uses/Configurations/Models/Accessories are not cleared for U.S. Surgery
INSTRUCTIONS TO THE AUTHORS FOR PUBLICATION IN BJ KINES-NATIONAL JOURNAL OF BASIC & APPLIED SCIENCE
 INSTRUCTIONS TO THE AUTHORS FOR PUBLICATION IN BJ KINES-NATIONAL JOURNAL OF BASIC & APPLIED SCIENCE BJ Kines-National Journal of Basic & Applied Science is a biannually (June Dec) publication of the B.
INSTRUCTIONS TO THE AUTHORS FOR PUBLICATION IN BJ KINES-NATIONAL JOURNAL OF BASIC & APPLIED SCIENCE BJ Kines-National Journal of Basic & Applied Science is a biannually (June Dec) publication of the B.
Astigmatism: analysis and synthesis of the astigmatic ametropia
 http://eoftalmo.org.br OPINION OF SPECIALISTS Astigmatism: analysis and synthesis of the astigmatic ametropia Astigmatismo: análise e síntese da ametropia astigmática Analysis and synthesis of the astigmatic
http://eoftalmo.org.br OPINION OF SPECIALISTS Astigmatism: analysis and synthesis of the astigmatic ametropia Astigmatismo: análise e síntese da ametropia astigmática Analysis and synthesis of the astigmatic
Mechanical aspects, FEA validation and geometry optimization
 RF Fingers for the new ESRF-EBS EBS storage ring The ESRF-EBS storage ring features new vacuum chamber profiles with reduced aperture. RF fingers are a key component to ensure good vacuum conditions and
RF Fingers for the new ESRF-EBS EBS storage ring The ESRF-EBS storage ring features new vacuum chamber profiles with reduced aperture. RF fingers are a key component to ensure good vacuum conditions and
JOURNAL OF PHARMACEUTICAL RESEARCH AND EDUCATION AUTHOR GUIDELINES
 SURESH GYAN VIHAR UNIVERSITY JOURNAL OF PHARMACEUTICAL RESEARCH AND EDUCATION Instructions to Authors: AUTHOR GUIDELINES The JPRE is an international multidisciplinary Monthly Journal, which publishes
SURESH GYAN VIHAR UNIVERSITY JOURNAL OF PHARMACEUTICAL RESEARCH AND EDUCATION Instructions to Authors: AUTHOR GUIDELINES The JPRE is an international multidisciplinary Monthly Journal, which publishes
Broken Wires Diagnosis Method Numerical Simulation Based on Smart Cable Structure
 PHOTONIC SENSORS / Vol. 4, No. 4, 2014: 366 372 Broken Wires Diagnosis Method Numerical Simulation Based on Smart Cable Structure Sheng LI 1*, Min ZHOU 2, and Yan YANG 3 1 National Engineering Laboratory
PHOTONIC SENSORS / Vol. 4, No. 4, 2014: 366 372 Broken Wires Diagnosis Method Numerical Simulation Based on Smart Cable Structure Sheng LI 1*, Min ZHOU 2, and Yan YANG 3 1 National Engineering Laboratory
Lin Liu, Jun Zou *, Hui Huang, Jian-guo Yang and Shao-rong Chen
 Liu et al. Diagnostic Pathology 2012, 7:55 RESEARCH Open Access The influence of corneal astigmatism on retinal nerve fiber layer thickness and optic nerve head parameter measurements by spectral-domain
Liu et al. Diagnostic Pathology 2012, 7:55 RESEARCH Open Access The influence of corneal astigmatism on retinal nerve fiber layer thickness and optic nerve head parameter measurements by spectral-domain
High Resolution Multicolor Contrast Scanner. Dimensioned drawing
 Specifications and description KRTM 20 High Resolution Multicolor Contrast Scanner Dimensioned drawing en 01-2011/06 50116669 12mm 20mm 50mm 12-30 V DC 50 / 25 khz We reserve the right to make changes
Specifications and description KRTM 20 High Resolution Multicolor Contrast Scanner Dimensioned drawing en 01-2011/06 50116669 12mm 20mm 50mm 12-30 V DC 50 / 25 khz We reserve the right to make changes
Intelligent Pendulum Hardness Tester BEVS 1306 User Manual
 Intelligent Pendulum Hardness Tester BEVS 1306 User Manual Please read the user manual before operation. PAGE 1 Content 1. Company Profile... 3 2. Product Introduction... 3 3. Operation Instruction...
Intelligent Pendulum Hardness Tester BEVS 1306 User Manual Please read the user manual before operation. PAGE 1 Content 1. Company Profile... 3 2. Product Introduction... 3 3. Operation Instruction...
DOSE DELIVERY SYSTEM OF THE VARIAN PROBEAM SYSTEM WITH CONTINUOUS BEAM
 DOSE DELIVERY SYSTEM OF THE VARIAN PROBEAM SYSTEM WITH CONTINUOUS BEAM EUCARD 2 WORKSHOP ON INNOVATIVE DELIVERY SYSTEMS IN PARTICLE THERAPY TORINO, 23 25 FEB 2017 VARIAN PARTICLE THERAPY HOLGER GÖBEL MANGER
DOSE DELIVERY SYSTEM OF THE VARIAN PROBEAM SYSTEM WITH CONTINUOUS BEAM EUCARD 2 WORKSHOP ON INNOVATIVE DELIVERY SYSTEMS IN PARTICLE THERAPY TORINO, 23 25 FEB 2017 VARIAN PARTICLE THERAPY HOLGER GÖBEL MANGER
Characterization and improvement of unpatterned wafer defect review on SEMs
 Characterization and improvement of unpatterned wafer defect review on SEMs Alan S. Parkes *, Zane Marek ** JEOL USA, Inc. 11 Dearborn Road, Peabody, MA 01960 ABSTRACT Defect Scatter Analysis (DSA) provides
Characterization and improvement of unpatterned wafer defect review on SEMs Alan S. Parkes *, Zane Marek ** JEOL USA, Inc. 11 Dearborn Road, Peabody, MA 01960 ABSTRACT Defect Scatter Analysis (DSA) provides
Guide to contributors. 1. Aims and Scope
 Guide to contributors 1. Aims and Scope The Acta Anaesthesiologica Belgica (AAB) publishes original papers in the field of anesthesiology, emergency medicine, intensive care medicine, perioperative medicine
Guide to contributors 1. Aims and Scope The Acta Anaesthesiologica Belgica (AAB) publishes original papers in the field of anesthesiology, emergency medicine, intensive care medicine, perioperative medicine
OPTOMETRY INVITED REVIEW. A review of astigmatism and its possible genesis
 C L I N I C A L A N D E X P E R I M E N T A L OPTOMETRY INVITED REVIEW A review of astigmatism and its possible genesis Clin Exp Optom 2007; 90: 1: 5 19 Scott A Read PhD Michael J Collins PhD Leo G Carney
C L I N I C A L A N D E X P E R I M E N T A L OPTOMETRY INVITED REVIEW A review of astigmatism and its possible genesis Clin Exp Optom 2007; 90: 1: 5 19 Scott A Read PhD Michael J Collins PhD Leo G Carney